
PAHO has focused growing attention on strategic planning to advance key regional and global health goals and as a means to improve its own performance. In 2007�2008, strategic planning was central to PAHO�s work, both as an area of technical cooperation and internally for the Organization itself.
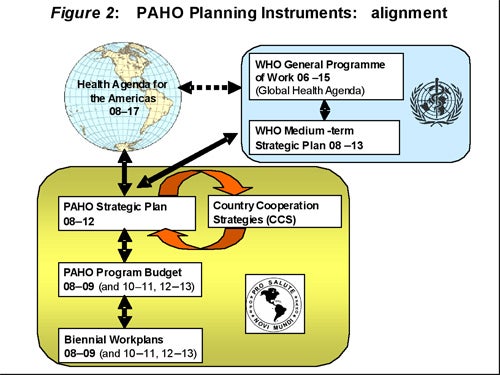
One of the highlights of 2007�2008 was the approval by the 27th Pan American Sanitary Conference of the PAHO Strategic Plan 2008�2012 (official document 328), a five-year framework for PAHO operations. The plan is based on the priorities and objectives laid out in the Health Agenda for the Americas 2008�2017 as well as on WHO�s 11th General Program of Work and Medium-Term Strategic Plan. Development of the PAHO Strategic Plan began in 2006 and was a participatory process that received inputs from PAHO�s Member States, Country Offices, centers, and technical and administrative areas.
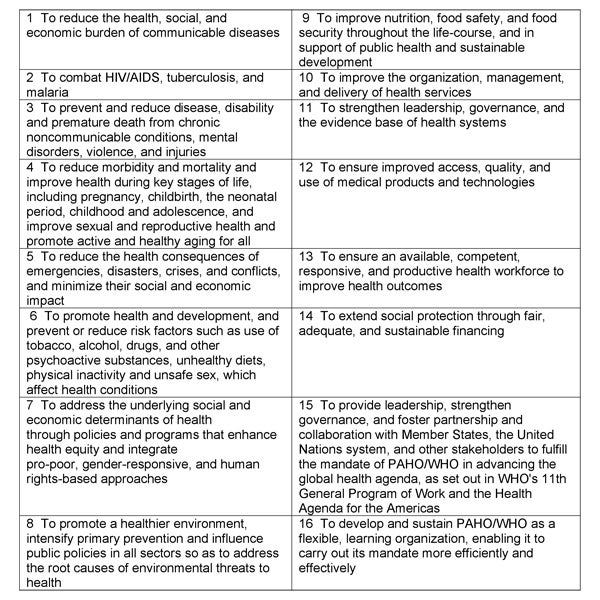
The PAHO Strategic Plan 2008�2012 is based on the results-based management framework that has been adopted by WHO and other U.N. agencies as part of the United Nations reform process. The plan sets forth 16 strategic objectives (SOs), a detailed implementation strategy, and expected results and indicators for measuring progress toward their achievement (regionwide expected results, RERs, and office-specific expected results, OSERs). To ensure transparency, the plan uses objectives and indicators for which baseline data are available at the start of the planning period. To ensure feasibility, it specifies both the resources needed and the expected sources of those funds. A revised version of the plan, which is being presented to the 48th Directing Council, incorporates new suggestions from Member States as well as adaptations of some indicators and goals and a new RER on climate change to ensure alignment with the new version of WHO�s Medium-term Strategic Plan 2008�2013.
Figure 1. Strategic Objectives, PAHO Strategic Plan 2008�2012
Through the development and implementation of the Strategic Plan, PAHO made significant progress during 2007�2008 in aligning its activities with the priorities and needs of its major constituents. The eight action areas of the Region�s Health Agenda for the Americas were a major input for the preparation of the Strategic Plan. PAHO Country Offices throughout the Region have begun or completed the preparation of country cooperation strategies (CCSs), which are directly linked to their biennial work plans and take into account country-specific needs as well as the United Nations Development Assistance Framework (UNDAF) and Common Country Assessments (CCA) (see Chapter 2). PAHO made special efforts to ensure that its designated priority countries-Bolivia, Guyana, Haiti, Honduras, and Nicaragua-were among the first to develop CCSs during 2007�2008. (In the case of Haiti, an Interim Cooperation Framework was developed instead). Particularly in these priority countries, the CCS process has facilitated the mobilization of additional resources for health.

PAHO�s U.S.�Mexico Border Office in El Paso, Texas, provides an example of the processes of planning and alignment that took place throughout the Organization during 2007�2008.
In March 2008, the secretaries of health of Mexico and the United States and PAHO�s Director signed a statement agreeing to jointly address mutual priorities in border health. The parties then established a Working Group made up of representatives of the U.S. Department of Health and Human Services, the Ministry of Health of Mexico, the U.S.-Mexico Border Health Commission (USMBHC), and PAHO. The Working Group developed an integrate framework to align the priorities and work plans of the USMBHC and PAHO�s U.S.�Mexico Border Office with the priorities agreed upon by the two countries. The framework includes a background statement describing each organization�s mission and vision and a review of the issues and challenges facing the communities along the U.S.�Mexico border.
Through a series of meetings, the Working Group developed a matrix detailing elements of the Border Office�s biennial work plan, the USMBHC�s �Directions and Priorities,� and suggested alignment actions within the two Organizations� project areas. The group also developed two additional matrices suggesting alignment actions for the short and medium terms. Subsequently, several agreements have been signed committing Mexican and U.S. government funds and committing PAHO and the USMBHC to maximizing the use of collective and individual resources to support their joint work.
A key feature of the PAHO Strategic Plan�s results-based management framework is its method for resource programming. The expected results are based on outcomes that are considered desired and feasible. The plan estimates the amount of resources needed to achieve 100 percent of those results and then allocates resources known to be available. Gaps between the available funding and the costs of the expected results will either leave them partially unmet or may be reduced by mobilizing additional resources.
As part of the results-based management environment, PAHO promotes staff development as a critical means of improving efficiency and effectiveness, enhancing technical excellence, and better focusing services to Member States. For this purpose, PAHO has developed a Learning Plan 2008�2012, which targets core learning content to staff throughout PAHO to help them build knowledge, skills, and competencies in specific areas. The Learning Plan supports the 16 Strategic Objectives of the PAHO Strategic Plan, the Country Cooperation Strategies, and special Target Areas of Capacity Building, which are derived from key mandates, including the Health Agenda for the Americas, the Millennium Development Goals, and WHO�s Six-Point Agenda to Improve Public Health.
PAHO has been a strong proponent of planning in public health since at least 1958, the year Chilean epidemiologist Abraham Horwitz became the Organization�s Director. Influenced by the emerging field of development economics, Horwitz and his contemporaries saw planning as an important instrument for promoting national development, and public health as an essential component of development.
The 1961 Charter of Punta del Este, which launched the Alliance for Progress, set forth an ambitious Ten-Year Public Health Program that aimed to increase life expectancy by 5 years over the decade through specific achievements in water and sanitation, child health, communicable disease control, nutrition, health services, and scientific research. Horwitz offered PAHO as the lead technical cooperation agency for the Regional plan and called on the Center for Economic and Social Development Studies (CENDES) at the Central University of Venezuela to develop a methodology for national and regional health planning. The PAHO promoted the CENDES methodology through training programs offered at its Pan American Center for Health Planning in Santiago, Chile. In 1971, a PAHO assessment showed considerable progress toward the goals of the 10-year plan but also significant differences in achievements across countries. At their 1972 meeting, the Region�s ministers of health reviewed lessons learned from the first 10-year plan and concluded that a lack of explicit policies on developing health systems had weakened the effectiveness of planning. In resolutions, they declared health as a universal right, acknowledged the importance of social participation in decision-making, and presented a new Ten-Year Health Plan (1971�1980) that focused on extending health services to underserved populations.

By the late 1970s, public health leaders in the Region and elsewhere had turned their focus from 10-year regional plans to primary health care strategies as the best way to guarantee health as a universal right. This process culminated in the 1978 Alma-Ata call for �health for all by the year 2000.� By 1980, most of the Region�s countries had developed national strategies to achieve �health for all by 2000,� and these became the basis for a set of Regional Strategies approved by the PAHO Directing Council. They set ambitious targets directly related to health for all, including the immunization of all children under 1 and the provision of water and sanitation services to the entire population, both by the year 1990. In 1981, PAHO adopted a Plan of Action to pursue these goals, with an emphasis on restructuring and expanding health services to increase equity, efficiency, and effectiveness.
The economic crisis of the 1980s resulted in fewer people, not more, having access to health services. In response, the 1988 PAHO Directing Council called for developing and strengthening local health systems as the basis for transforming national health systems. The approach was intended to promote citizen participation in health promotion and the delivery of services, thereby increasing accountability.
By 1990, the Pan American Sanitary Conference had developed a host of new and continuing strategic orientations to guide the work of PAHO and its Member States. These included attention to the role of health in development, reorganizing the health sector, focusing on high-risk groups, health promotion, social communication, integrating women in health and development, knowledge management, resource mobilization, and technical cooperation among countries.
Today, planning is for PAHO a key means for ensuring effective health action in the Americas. The new PAHO Strategic Plan 2008�2017 is highly integrated and carefully articulated to link with its external mandates, with operationally well-defined indicators, baselines, and targets to ensure that the results of Organization�s efforts are meaningful and measurable. The plan reflects PAHO�s commitment, in conjunction with other U.N. agencies and international cooperation institutions, to ensuring that its work is efficient and effective, and that the Organization is ultimately accountable to the people it is intended to serve.
In line with WHO, PAHO has taken measures to ensure that its administrative processes and information systems also support the new strategic direction and commitment to its Member States. As part of this process, PAHO is using WHO�s Global Management System (GSM) and its guiding principles as a compass to maintain programmatic alignment with WHO while respecting PAHO�s separate governance structure and legal status. This will ensure that PAHO provides the required programmatic and financial data to WHO for integration into its global program planning and reporting processes while also responding to the Organization�s regional requirements.
In 2007, the PASB made major advances in its program management and budget systems. The Organization�s key managerial instrument, AMPES/OMIS, was enhanced with the addition of a new web-based budget module, the Award Management System (AMS). In alignment with the GSM guiding principles, the new AMS is configured to 1) enable managerial entities to develop biennial work plans linked to the Organization�s Strategic Plan and Program Budget, and 2) facilitate the transition from a programmatic structure based on �areas of work� to one based on �strategic objectives.� The new system allows managerial entities to establish �office-specific expected results� with associated indicators that are directly linked with the �regionwide expected results� contained in the PAHO Strategic Plan. In this way, the system documents the contributions of all managerial entities to the achievement of the Organization�s strategic objectives.
In 2008, the PASB will finalize its implementation of a new Performance Monitoring and Assessment system to complete the new planning, programming, and management environment.
During 2007, PAHO mobilized significantly greater financial resources, enabling the Organization to strengthen its technical cooperation efforts. Total funding reached $620.8 million, the highest level of income for the Organization in any one year. Receipts of current and prior years� quota assessments totaled $68 million and $44.6 million, respectively. PAHO received $67.6 million from WHO, of which $39.2 million was for regular budget activities and $28.4 million was for extra-budgetary projects. The Organization also received $284.4 million to procure vaccines and other supplies on behalf of PAHO Member States.

PAHO mobilized $153.8 million in voluntary contributions, including $72.6 million from governments for external projects, $71.3 million from governments for domestic projects ($68.9 million from Brazil), $5 million from international organizations, $4.7 million from private and public sector organizations, and $197,000 from other sources. The largest contributors of voluntary funds were Brazil ($72.6 million), Canada ($16.3 million), Norway ($1.3 million), Spain ($23.3 million), Sweden ($5.7 million), the United Kingdom ($1.9 million), and the United States ($17.9 million).
PAHO�s financial management has responded proactively to this dramatic growth in financial resources as well as to decentralization and the implementation of results-based management. In 2006�2007, the Organization implemented a new Financial Accountability Framework, which included the review of financial policies and procedures, staff training, and a requirement that all Country Office representatives and senior managers at Headquarters certify their offices� annual financial accounts. A newly implemented Expenditure Recognition Policy and the expected implementation of International Public Sector Accounting Standards (IPSAS) in alignment with the United Nations and its specialized agencies will enhance PAHO�s commitment to results-based management. These initiatives will continue to position PAHO as a leader in financial best practices among both public and private sector institutions and will support the Organization�s continued commitment to its fiduciary responsibilities.
During 2007, PAHO received approval from its Governing Bodies to implement a Master Capital Investment Plan (MCIP). Historically, PAHO had addressed the requirements for property, plant, and equipment, as well as IT-related infrastructure, on an ad-hoc basis. With the advent of the MCIP, the Organization will regularize the planning process and address maintenance and infrastructure needs in a more deliberative manner over a 10-year period. The MCIP will be continuously updated on a rolling 10-year cycle and incorporated into the Biennial Program Budget planning and funding process.
The $8 million initial funding for the MCIP was provided from the excess of income over expenditure in the 2006�2007 Regular Program Budget. Future financing will come from excesses of income over expenditure, if available, in the Regular Program Budget at the end of each biennium. PAHO has been approached to provide assistance to other United Nations agencies in establishing this best budgetary and financial practice.