Syphilis is a bacterial infection caused by Treponema pallidum that results in substantial morbidity and mortality. Syphilis is a sexually transmitted infection (STI) usually spread among humans through contact with infectious sores on the genitals, anus, rectum, lips or mouth, via blood transfusion. It can also be transmitted through mother-to-child transmission during pregnancy (congenital syphilis).
Correct and consistent use of condoms significantly decreases the risk of infection. Mother-to-child transmission of syphilis (congenital syphilis) is preventable and can be achieved through early screening and treatment among pregnant women.
Congenital syphilis can be easily prevented by early detection, prompt and adequate treatment of infected pregnant women.
Syphilis diagnosis is usually based on medical history, physical examination, and laboratory testing. Uncomplicated syphilis can be easily cured with antibiotics, however if left untreated, the disease last for years and cause serious health problems.
This is one of the 30 conditions that the Elimination Initiative has proposed to eliminate in the Region of the Americas by the year 2030.
- Symptoms vary depending on the different stages of syphilis. Symptoms usually begin 21 days after infection but can range from 9 to 90 days. In many cases syphilis does not cause symptoms.
- If a pregnant woman has syphilis, it can be transmitted to the baby. Mother-to-child transmission of syphilis can be prevented by early detection and treatment with the appropriate antibiotic (benzathine penicillin).
- Approximately 40% of babies born to pregnant women with untreated syphilis can be stillborn or die from the infection.
- Syphilis can in most cases be easily cured with antibiotics (penicillin). A fetus can also be easily cured with treatment, and the risk of adverse outcomes to the fetus is minimal if the mother receives adequate treatment during early pregnancy – ideally before the second trimester.
- Untreated syphilis increases the risk of transmitting or acquiring HIV by two or three times in some populations.
- Syphilis disproportionately affects some population groups such as men who have sex with men (MSM), trans women and female sex workers.
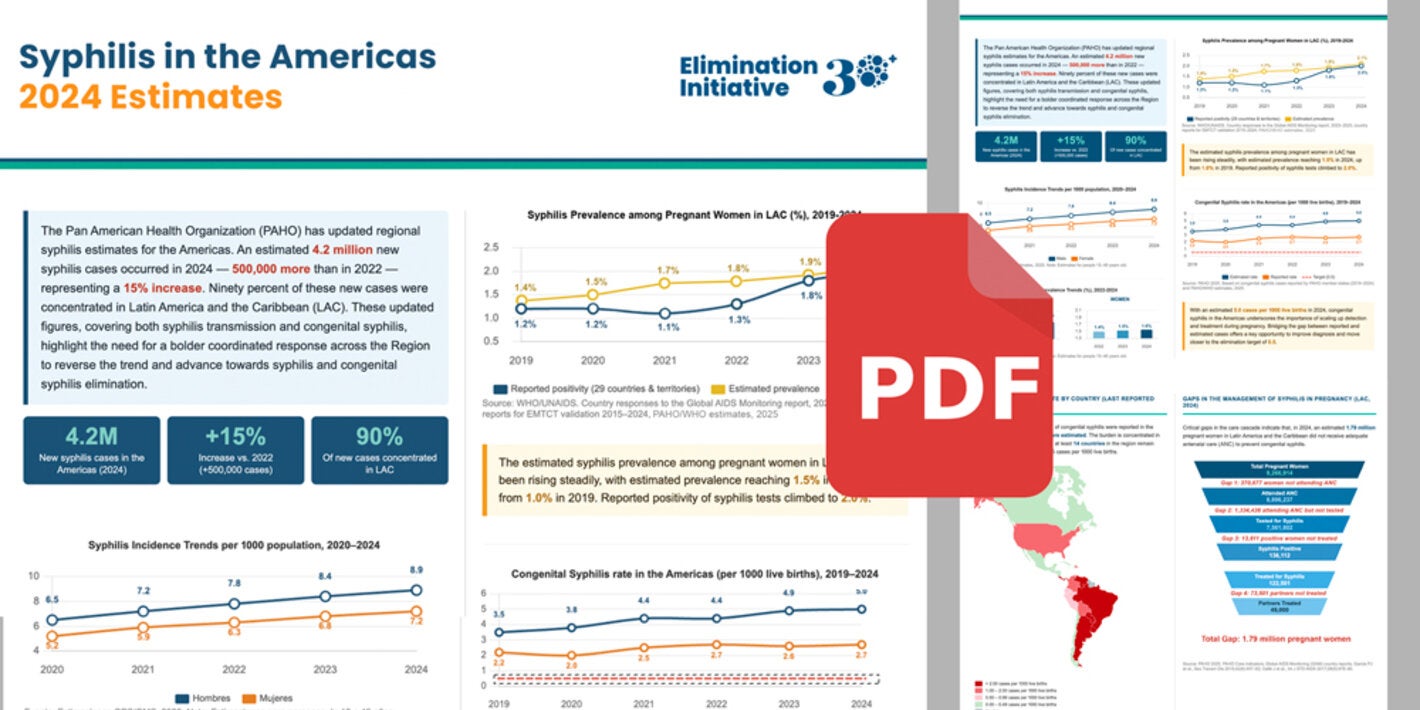
- In recent years, syphilis infections have increased in the Americas. This increase has also occurred in pregnant women resulting in an increase in cases of congenital syphilis.
Syphilis is a sexually transmitted infection (STI) caused by a bacterium. If left untreated, the disease last for years and can cause serious health problems. Syphilis is divided into four stages. Early syphilis consists of primary syphilis, secondary syphilis and early latent syphilis, while late syphilis consists of late latent syphilis and tertiary syphilis.
You can get syphilis by having direct sexual contact with infectious sores (chancre) on the genitals, anus, rectum, lips or mouth through unprotected vaginal, anal, or oral sex with someone who has syphilis. You can still get syphilis even if you had it in the past and got treatment for it. Sexual transmission typically occurs during primary, secondary or early latent stage infections. Syphilis can also be spread via blood transfusions. Around 50% of pregnant women with untreated syphilis will spread the infection to their unborn child.
Correct and consistent use of condoms significantly decreases the risk of infection. If the sores occur in an area not covered by the condom transmission can still occur. Congenital syphilis is preventable through early screening and immediate treatment for syphilis in pregnant women.
Symptoms vary depending on the different stages of syphilis. Symptoms usually begin 21 days after infection but can range from 9 to 90 days. Primary syphilis usually presents as a single, painless sore (chancre) at the site of inoculation. The primary chancre can go unnoticed.
If untreated, the disease progresses to the secondary stage that can cause skin rashes, fever, and swollen lymph nodes. The rash of secondary syphilis can vary widely and mimic other infectious or non-infectious conditions, but characteristically affects the palms and soles. The rash is often symmetrical and non-itchy, but may have several manifestations and can be minimal enough to be overlooked. In warm and moist areas of the body, such as the anus and labia, large white or grey raised lesions develop as a result of the spread of the treponemes from the primary lesion. The symptoms and signs of secondary syphilis naturally resolve, even without treatment, but if left untreated, the patient enters the latent stage.
In the latent stage, which can last for years, the bacteria are still present in the body, but there are no symptoms or signs. Most patients will remain in the latent stage if left untreated, while around 25% will develop tertiary syphilis. The main manifestations of tertiary syphilis are neurological disease (neurosyphilis), cardiovascular disease (cardiosyphilis) and granuloma (gummatous lesions or gumma). Tertiary syphilis can affect any organ system up to 30 years or more after infection and can be life- threatening.
Neurosyphilis can occur at any stage of syphilis infection, even in the first few months. Early neurological manifestations include acute changes in mental status, meningitis (inflammation of the membranes surrounding your brain and spinal cord), stroke, cranial nerve dysfunction and auditory or ophthalmic and ocular abnormalities.
Mother-to-child transmission may occur if the expectant mother has syphilis. Mother-to-child transmission of syphilis (congenital syphilis) is usually devastating to the fetus in cases where maternal infection is not detected and treated sufficiently early in pregnancy.
If syphilis is left untreated during pregnancy it can lead to early birth, low birth-weight, stillbirth, death shortly after birth or other sequelae in the baby, including inflammatory manifestations affecting the eyes, ears and joints, as well as skeletal malformations resulting from developmental damage during the early stages of syphilis.
It is important to keep in mind that many infants with syphilis infection may not have obvious clinical signs or symptoms. Mother-to-child transmission of syphilis is preventable and can be achieved through early screening and treatment with the right antibiotic (penicillin).
Syphilis diagnosis is usually based on medical history, physical examination, and laboratory testing. Point-of-care rapid diagnostic tests (RDTs) for syphilis infection screening can provide results in 10–15 minutes and can be performed in any setting since they do not require refrigerated storage or laboratory equipment. Currently, WHO recommends the use, in pregnant women, of a dual RDT to screen for both HIV and syphilis infections. However, a positive result from a syphilis RDT does not distinguish between active infection and previously treated infections but it is an important resource for treatment initiation particularly among pregnant women and hard to reach populations. PDRs that can detect both active and past syphilis infection are now available.
For more information see WHO guideline on syphilis screening and treatment for pregnant women.
Syphilis can in most cases be easily cured with antibiotics (penicillin). A fetus can also be easily cured with treatment, and the risk of adverse outcomes to the fetus is minimal if the mother receives adequate treatment during early pregnancy – ideally before the second trimester. For detailed information on recommended treatment, see WHO guidelines for the treatment of syphilis.
- The global response to STIs currently follows the guidelines of the Global health sector strategies on, respectively, HIV, viral hepatitis, and sexually transmitted infections for the period 2022-2030.
- This strategy outlines strategic lines of action for Member States and the Pan American Sanitary Bureau to implement to improve and expand the prevention and control of HIV infection, viral hepatitis and STIs.
- PAHO/WHO has expanded the plan of action to include EMTCT Plus, leveraging the maternal and child health platform to include elimination of other preventable communicable diseases in the Americas, such as hepatitis B and Chagas disease.
- PAHO/WHO develops guidelines and handbooks to support countries improving surveillance, prevention, diagnosis and treatment of STI, including PAHO’s 2015 Guidance on Syphilis Testing in Latin America and the Caribbean: Improving Uptake, Interpretation, and Quality of Testing in Different Clinical Settings.
- In 2016, WHO developed the Guidelines for the Treatment of Treponema pallidum (syphilis), and in 2017 the Guideline on syphilis screening and treatment for pregnant women, both providing updated recommendations for syphilis based on the most recent evidence.
- PAHO works with countries in the Americas to improve syphilis surveillance and strengthen the capacities of prenatal care personnel for syphilis and congenital syphilis. PAHO also collaborates with local communities and civil society to advocate and promote the elimination of these diseases. Both syphilis and congenital syphilis are included in PAHO's Elimination Initiative, which aims to end more than 30 diseases and related conditions by 2030.
- This technical note consolidates World Health Organization (WHO) recommendations for the prevention and control of syphilis and congenital syphilis. It shares best practices from different countries in the Americas to implement these recommendations. It also provides WHO recommendations for surveillance and monitoring of syphilis and congenital syphilis. Finally, it details the supplies for the diagnosis and treatment of the disease, available through the Strategic Fund of the Pan American Health Organization.